

Closing the Loop: The Latest on Artificial Pancreases
20 July 2024
Closed-loop insulin delivery systems, also known as artificial pancreas systems, are currently in an exciting phase of technological innovation and transformation, and look set to transform the management of diabetes for the future. These innovations are driven by enhancements in sensing and delivery technology, promising clinical trial results, and new regulatory approvals.
The development and provision of these systems is currently focused on people with Type 1 Diabetes (T1D). People with T1D have an immune system that attacks the β cells in the pancreas which create insulin, a hormone which enables the transport of that glucose from the bloodstream to the rest of the body. Most of the insulin produced by a healthy β cell is a reaction to the current level of glucose in the bloodstream, however some is even produced by the body during chewing in preparation for a blood sugar spike.1
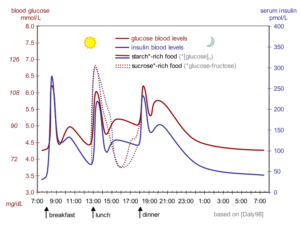
Figure 1: Insulin levels in the blood of a healthy human, showing the sensitivity required to maintain a healthy blood sugar level over the course of the day.2
People with T1D must inject insulin to manage their blood glucose levels over the course of the day. With a manual system, calculation of the required insulin dose can be a complex process, requiring patients to constantly monitor glucose levels and use that information to plan and execute calculations at specific times.2 The effect of a certain dose of insulin even has its own day-to-day variability, which is difficult to predict. Most people with T1D are therefore not able to achieve their recommended glycaemic targets.3
Artificial pancreas systems aim to bring management of T1D into the digital era. The essential components are a continuous glucose monitor (CGM), an insulin pump and a control algorithm. Most systems are known as ‘hybrid’, meaning that even though insulin rate is adjusted automatically, users still have some interaction with the system, for example counting and entering mealtime carbohydrates.4

Figure 2: The key components of an artificial pancreas system.6
A SPIKE IN PRECISION
CGMs measure glucose levels in the interstitial fluid between cells in the abdomen or back of the upper arm, normally via an enzymatic reaction. There is an inherent delay of approximately 10 minutes5 in the reading when measuring blood glucose in this way, which affects the accuracy of the reading and thus the performance of the control algorithm.
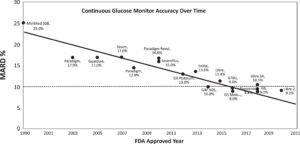
Figure 3: Improvements in CGM MARD since 1990.9
| FDA approval (year) | CE mark (year) | MARD (%) | Warm up time (hours) | Service life (days) | |
| Abbott FreeStyle Libre 3 | 2022 | 2022 | 7.9 | 1 | 14 |
| Dexcom G7 | 2022 | 2020 | 8.2 | 0.5 | 10 |
Table 1 – Technical details of the most recently approved CGMs
As shown in Table 1 above, the newest CGMs can achieve a mean absolute relative difference (MARD) of 8% when compared to a calibrated reference, report glucose levels every minute, and do not require any calibration by the user by way of a fingerstick reading. The impressive accuracy of current monitors is the result of year-on-year performance improvements as can be seen in Figure 1, where an MARD of <10% is considered accurate enough for insulin dose calculations.6 It is currently unclear whether the accuracy of new sensors will continue to improve or begin to flatten out as we approach the limit of the technology.
Further development work in this area is also ongoing to ensure that the accuracy of the CGM is maintained over a range of use cases. For example, compression of the device when sleeping and long periods of aerobic exercise have been shown to produce erroneous readings. There are also efforts to reduce the effects of various interfering substances such as ascorbic acid, hydroxyurea, and others yet to be identified.7
SMART PUMPS AND APPS
The control algorithm can either be integrated into the pump itself or located on a separate device, which can even be a smartphone. The safety of the control system is paramount, as delivering too much insulin can cause hypoglycaemia which can quickly become life threatening if untreated.
The three main types of control algorithms used in approved systems are:
- Proportional-integral-derivative (PID) – One of the most common control methods, a predefined proportional, integral and derivative equation use an error value in parallel to make frequent corrections. A pump using this algorithm is therefore more dependent on live blood sugar readings to make frequent adjustments. Artificial pancreases using PID usually also incorporate an insulin feedback (IFB) algorithm to account for the effect that current insulin levels in blood plasma suppress insulin secretion from β-cells in healthy humans quicker than the system can account for when measuring interstitial blood sugar levels with a CGM.8
- Fuzzy logic (FL) – Used in the new MiniMed 780G in conjunction with PID control, fuzzy logic mimics human vagueness in decision making when working with incomplete data. This improves the algorithm’s response to unexpected situations such as illness, exercise, or unannounced meals.9
- Model predictive control (MPC) – Generally regarded as a more advanced method of control, where new predictive models over a defined ‘horizon’ are rapidly generated and updated as blood sugar levels change. It is therefore considered better for systems like artificial pancreases that have large time delays or predictable dynamics. However, as with PID the algorithm may require additional controls to deal with disturbances that break from the models.
| Pump | FDA approval (year) | CE mark (year) | Algorithm | CGM compatibility | |
| Medtronic | MiniMed 670G | 2016 | 2018 | PID with IFB | Medtronic Guardian 3 |
| MiniMed 770G | 2020 | PID with IFB | Medtronic Guardian 3 | ||
| MiniMed 780G | 2023 | 2020 | PID with IFB & FL | Medtronic Guardian 4 | |
| Tandem | t:slim X2 with Control-IQ | 2022 | 2018 | MPC | Dexcom G6/G7 |
| Insulet | Omnipod | 2022 | 2024 | MPC | Abbott FreeStyle Libre 3
Dexcom G6 |
| BetaBionics | iLet Bionic Pancreas | 2023 | MPC | Dexcom G6/G7 | |
Table 2 – A summary of approved hybrid closed-loop systems for Type 1 diabetes in Europe & the US, where the control algorithm is on the pump
Most of the artificial pancreas systems in Table 2 above are now approved in both the EU and US. Medtronic, the first entry into the market, operate within a closed ecosystem, whereas newer entries by competitors typically use Dexcom and/or Abbott CGMs. This potentially gives users more choice and reduce any chance of geographical supply limitations. On the other hand, Medtronic’s ownership of the whole ecosystem could allow them to be closer to the sensor technology and implement improvements in sensor technology directly into their own algorithm.
| Description | CE mark (year) | Algorithm | Pump compatibility | CGM compatibility | |
| Diabeloop DBLG1 | Purpose-built touchscreen handset using Android | 2018 | MPC | ViCentra Kaleido
Roche Accu-Chek Insight |
Dexcom G6 |
| CamDiab CamAPS FX | App available for Android and iOS | 2022 | MPC | Ypsomed mylife YpsoPump
Advanced Therapeutics DANA Diabecare RS and DANA-i |
Abbott FreeStyle Libre 3
Dexcom G6 |
Table 3 – A summary of approved hybrid closed-loop systems for Type 1 diabetes, currently only approved in Europe, where the control algorithm is on a separate device
As for the systems in Table 3 above, placing the controller on a separate device increases the potential for device interoperability but have other trade-offs. In the case of the Diabeloop, the user must carry another handheld device with them. As an Android/iOS app, CamAPS FX does not have this problem for most users, but could leave diabetes management vulnerable to typical problems with apps, such as problems arising when using specific smartphones and OS versions.
#WEARENOTWAITING
There are currently thousands of people around the world currently using some form of DIY closed loop system.10 The movement has centred around the hashtag #WeAreNotWaiting, with the intention of improving the availability and affordability of artificial pancreas systems. For example, in the US a new insulin pump and transmitter can cost up to $7400, not including $420 for a 30-day supply of sensors.11 Last year it was announced that that hybrid closed loop systems would be made available for UK NHS patients over the next 5 years.12
The three main DIY artificial pancreas systems in use are:
- OpenAPS, the first system to be developed in 2016 using a Raspberry Pi to control a set of now unsupported Medtronic pumps released between 2003 and 2010.
- Loop, a similar approach but designed work on the iPhone. It is compatible with the same Medtronic pumps as OpenAPS with the addition of the Omnipod.
- AndroidAPS, which has the same functionality of OpenAPS but can be installed on an Android smartphone.
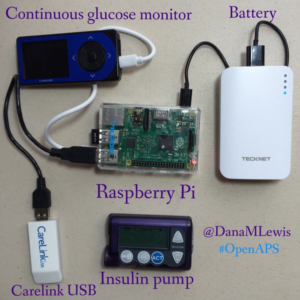
Figure 4: A DIY artificial pancreas system from 2016, using a battery-powered Raspberry Pi, Dexcom receiver, and CareLink USB stick transmitting to a Medtronic pump.16
Interestingly, these systems are not based on any of the advanced control algorithms mentioned in the previous section, but rather designed to emulate the decision-making process that a user would manually step through when using a bolus pump. They can also be configured to provide the exact amount of automation and responsiveness that works for a specific user. Some studies report similar performance for key metrics such as in time in range and HbA1c levels when compared with approved hybrid closed loop systems.13 However, creating a working DIY system requires some technical know-how.
In 2023, a diabetes non-profit charity called Tidepool received clearance from the FDA to go ahead with Tidepool Loop. This is an effort to bring an easier to use but open-source system into regulatory control. Unfortunately the system is currently not available for use, as it requires pump manufacturers to gain clearance from the FDA for their use with an alternative controller, which has not happened yet.14
THE FUTURE
The artificial pancreases of the future could develop in a number of ways. Control algorithms could improve, helping to overcome the time delay in sensing of blood sugar levels, and absorption and action of insulin. Machine learning and AI could play a key role in generating bespoke predictive models. Also, the introduction of ultra rapid acting insulin analogues like Fiasp (Novo Nordisk) and Lyumjev (Eli Lilly) could increase system responsiveness.15
People with T1D also have deficiencies producing other hormones that control blood sugar, such as glucagon. This hormone increases blood sugar levels from stores, so could allow for more aggressive insulin dosage during spikes while reducing the risk of hypoglycaemia. Subtle pancreatic regulators such as amylin analogues (pramlintide) and GLP-1 agonists could also be added to the mix. Every new development in the artificial pancreas story has been an exciting step forwards, and it is clear that this trend will continue long into the future.
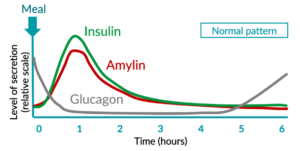
Figure 5: The opposing roles of insulin and glucagon in the regulation of blood glucose levels.20
Written by Kamaal de Silva, Principal Mechanical Engineer, Springboard and featured in On Drug Delivery.
REFERENCES:
- Eliasson B, Rawshani A, Axelsen M, Hammarstedt A, Smith U. Cephalic phase of insulin secretion in response to a meal is unrelated to family history of type 2 diabetes. PLoS One. 2017;12(3):e0173654. doi:10.1371/journal.pone.0173654
- Vloemans AF, Eilander MMA, Rotteveel J, et al. Youth With Type 1 Diabetes Taking Responsibility for Self-Management: The Importance of Executive Functioning in Achieving Glycemic Control. Diabetes Care. 2019;42(2):225-231. doi:10.2337/dc18-1143
- Davies M. The reality of glycaemic control in insulin treated diabetes: defining the clinical challenges. Int J Obes. 2004;28(S2):S14-S22. doi:10.1038/sj.ijo.0802745
- Story of Discovery—Artificial Pancreas for Managing Type 1 Diabetes: Cutting-edge Technology 50 Years in the Making – NIDDK. National Institute of Diabetes and Digestive and Kidney Diseases. Published January 24, 2017. Accessed November 29, 2023. https://www.niddk.nih.gov/news/archive/2017/story-discovery-artificial-pancreas-managing-type1-diabetes
- Schmelzeisen-Redeker G, Schoemaker M, Kirchsteiger H, Freckmann G, Heinemann L, del Re L. Time Delay of CGM Sensors: Relevance, Causes, and Countermeasures. J Diabetes Sci Technol. 2015;9(5):1006-1015. doi:10.1177/1932296815590154
- Kovatchev BP, Patek SD, Ortiz EA, Breton MD. Assessing Sensor Accuracy for Non-Adjunct Use of Continuous Glucose Monitoring. Diabetes Technology & Therapeutics. 2015;17(3):177-186. doi:10.1089/dia.2014.0272
- Friedman JG, Cardona Matos Z, Szmuilowicz ED, Aleppo G. Use of Continuous Glucose Monitors to Manage Type 1 Diabetes Mellitus: Progress, Challenges, and Recommendations. Pharmacogenomics and Personalized Medicine. 2023;16:263-276. doi:10.2147/PGPM.S374663
- Ruiz JL, Sherr JL, Cengiz E, et al. Effect of Insulin Feedback on Closed-Loop Glucose Control: A Crossover Study. J Diabetes Sci Technol. 2012;6(5):1123-1130
- Mauseth R, Hirsch IB, Bollyky J, et al. Use of a “fuzzy logic” controller in a closed-loop artificial pancreas. Diabetes Technol Ther. 2013;15(8):628-633. doi:10.1089/dia.2013.0036
- OpenAPS Outcomes – OpenAPS.org. Accessed May 19, 2024. https://OpenAPS.org/outcomes/
- Dermawan D, Kenichi Purbayanto MA. An overview of advancements in closed-loop artificial pancreas system. Heliyon. 2022;8(11):e11648. doi:10.1016/j.heliyon.2022.e11648
- New “artificial pancreas” technology set to change the lives of people having difficulty managing their type 1 diabetes | News | News. NICE. Published January 10, 2023. Accessed November 29, 2023. https://www.nice.org.uk/news/article/new-artificial-pancreas-technology-set-to-change-the-lives-of-people-having-difficulty-managing-their-type-1-diabetes
- Kesavadev J, Srinivasan S, Saboo B, Krishna B M, Krishnan G. The Do-It-Yourself Artificial Pancreas: A Comprehensive Review. Diabetes Ther. 2020;11(6):1217-1235. doi:10.1007/s13300-020-00823-z
- Downey L, O’Donnell S, Melvin T, Quigley M. A European regulatory pathway for Tidepool loop following clearance in the United States? Diabetic Medicine. 2024;41(4):e15246. doi:10.1111/dme.15246
- Hartnell S, Fuchs J, Boughton CK, Hovorka R. Closed-loop technology: a practical guide. Practical Diabetes. 2021;38(4):33-39. doi:10.1002/pdi.2350
